
What I've Learned from Consumers about Tobacco Harm Reduction
From language to research design to policy

The part of my last post that seemed to resonate with people the most was my call for consumer involvement in tobacco harm reduction (THR). I thought this was worth expanding into its own post:
To share some things that I (a recovering academic) personally do differently after talking with consumers
Discuss specific areas of research in which the lack of consumer involvement is most harmful (to consumers, public health, and research integrity)
Changes That I’ve Personally Made
Person-First Language
Many people — most prominently for me, Skip “Be Kind” Murray — have been campaigning for years to normalize person-centered language (“person who smokes”) instead of stigmatizing terms like “smoker”. As an insulated academic who has never smoked (except trying out of curiosity), I didn’t comprehend how bad the stigma was until I saw Skip post about the “wall of hate”. Not everyone agrees that this wording change will really reduce stigma, and many researchers (including myself at first) grumbled about how this introduces clunky language and makes it even more difficult to squeeze our research into journals’ word counts. But if it’s important to Skip, then it’s important to me.
This is one thing that’s improved noticeably over the past few years. More journals are now recognizing the importance of person-first language (see editorial in Nicotine & Tobacco Research by editor-in-chief Prof. Caitlin Notley), or even requiring it (e.g. Harm Reduction Journal; and section editor Prof. Marewa Glover is more than willing to have longer papers in order to accommodate person-first language). I now enforce this language when I do peer reviews, even if the journal does not have an explicit policy.
“Unintended” vs “indirect consequences”
I have gotten pushback from Miles Davis when I use phrases like “unintended consequences” or “X policy inadvertently increased smoking” and have seen many other consumers object to this language. The rationale is that there are perverse incentives to oppose THR — e.g. state and federal governments depend on cigarette excise taxes being a large part of their budget; academics depend on funding agencies that often have a stance hostile to THR (see my post on academic incentive structures).
I was a bit torn on this feedback because on one hand, I don’t like to attribute ill intent to what could just be naivety (as I well understand, having once been a naive academic myself who initially had no reason to question the established narrative that e-cigarettes were a public health threat). Accusing well-intentioned but naive academics and policymakers of intentionally trying to keep people smoking cigarettes is confrontational and not conducive to bridging the polarity in THR.
On the other hand, I do acknowledge that there are perverse incentive structures and think it’s important to point them out where they exist, whether or not there’s a conscious awareness that opposing reduced-risk nicotine products effectively serves to perpetuate cigarette smoking. I also think that the substitution effect between cigarettes and e-cigarettes is well-documented enough that these harmful policy effects shouldn’t be a complete surprise. I understand the sentiment that honest ignorance only gives so much leeway when anyone recommending policies should be doing their due diligence to ensure those policies won’t increase net harm. Especially when consumers repeatedly point out evidence for these harmful effects to tobacco control accounts on social media; they are frustrated because they feel their very legitimate concerns are being ignored.
My solution is to now say “indirect consequences” because that avoids assuming conscious intentions (either assuming ill intent or implying that naive good intentions absolves them of responsibility for harmful effects) while also more precisely describing the dynamics I’m referring to: that the policies are often aimed at a different thing (e.g. banning e-cigarette flavors or taxing e-cigarettes) which often achieve their direct effects but have harmful indirect effects.
Interpreting Behavioral Research
Most of my research involves analyzing behavioral data collected in surveys. Since my expertise is more on the analysis side, I usually come in at a later stage of the process, after others have designed the survey and collected the data. This has some limitations because I can’t ask any follow-up questions or ask for clarification if I’m confused by the constrained response options on a survey.
For example, sometimes it’s unclear how to categorize smoking status. A lot of the consulting work we do at Pinney in consulting to Juul is analyzing data from a large longitudinal survey of adult JUUL purchasers. We’ve published many papers from this study, with different papers focusing on different groups based on their smoking status at baseline. Our papers mostly focus on participants reporting current & established smoking at baseline, with some papers on former and never smoking (see the special issue of the American Journal of Health Behavior). But there’s one fairly sizeable group whose status was not really clear (from the article describing the overall methods of this study):
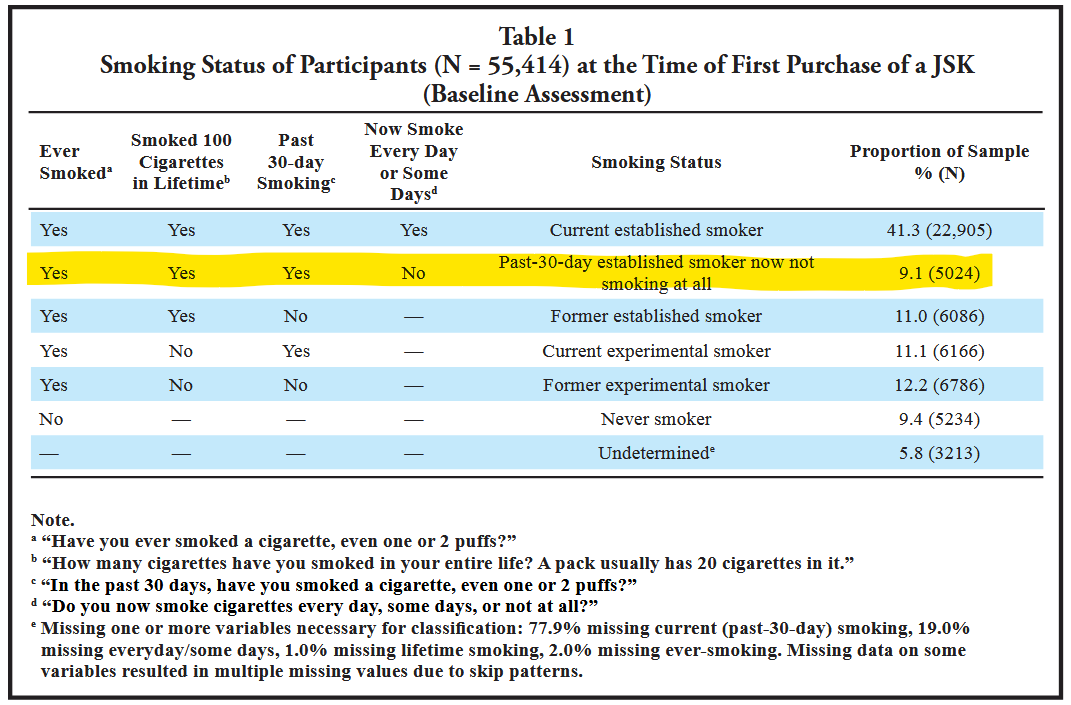
They were almost the same as the largest group (those reporting current, established smoking): they had smoked in the past month at baseline (which is sometimes the definition of “current smoking”) and had established smoking history (100+ cigarettes/lifetime), but this group reported smoking “not at all now” (versus some days or every day).
It’s not entirely clear what’s going on with this group: did they stop smoking very recently (within the past 3 weeks) or is this inconsistent/inattentive reporting that’s always present to some degree in every survey? My colleagues favored the former interpretation in the article above, based on additional analyses from PATH which had more granularity in the questionnaire:
Analyses of data form PATH (Supplement 2) suggest that these may be individuals who considered themselves to have stopped smoking more recently than 30 days ago.
In talking with consumers, this seems to be a valid interpretation (although a small proportion of this group may still be inconsistent responding). For example, Jukka Kelovuori described his process as a “clean switch,” i.e. he immediately stopped smoking after his first use of an e-cigarette. Others more gradually replaced more of their cigarettes with e-cigarettes until they realized they no longer smoked.
Because of the survey design — i.e. buying a Juul starter kit and then completing this survey within a week or two — any “clean switchers” would fall in the category of “past 30-day but ‘not at all now’ smoking.” For the papers where we analyzed rates of switching away from smoking, we didn’t include this group (since we weren’t completely sure what was going on in this group due to the limitations of the survey, i.e. not asking details of past-30-day smoking of anyone who said they smoked “not at all'“ now). But knowing that “clean switching” is a common enough phenomenon will factor into my interpretation of switching studies (i.e. true switching rates could be even higher) and it also highlights the need for improvements in future studies to better capture clean switching.
I’ve also learned a lot from consumers about why they use nicotine. I’ve always believed in freedom of choice: as long as people are informed about the risks and it’s not negatively impacting others, it should be up to them to evaluate the trade-off for them personally between the risks and the internal or subjective benefits they experience. Talking to consumers has taught me a lot about the latter side of the equation. Richard Pruen has written about how nicotine is the only substance that helps his ADHD symptoms without intolerable side effects that medications had for him:
I picked up a cigarette that somebody else had half smoked, took a few puffs, and suddenly, I could think in straight lines. It was that profound… I don’t think that I’d have made it through college if I didn’t smoke. It was that profound a change in just being able to focus on something.
Fortunately Richard switched to vaping. He still experiences benefits from using nicotine:
Well, I discovered that nicotine worked when I took up vaping in 2007. I started vaping seriously in 2008, but only in situations where I couldn’t light up a cigarette. By early March 2009, I’d quit smoking by accident… Around 2010, I tapered down nicotine, thinking, well, I’ll just stop vaping. And then it kicked in that nicotine is actually useful; it’s doing something.
Understanding this perspective helps explain why the use of any nicotine/tobacco product stay approximately stable despite drastic changes in which specific products are being used. This has happened in Norway and Sweden with snus (e.g. see my work with Dr. Karl Erik Lund on population trends in Norway) and are occurring in the US and elsewhere (e.g. this is shown well by Sanford et al. 2024). Which means that researchers and policymakers should expect a proportion of people to always use nicotine in some form and can’t reasonably expect policies to eliminate all nicotine use.
Public Science Communication
Academic writing is very esoteric and there’s a lot of lingo that is clear only to other academics, but the science is relevant to large proportions of the public and it’s important to communicate it. Since starting at Pinney I’ve become active on social media to communicate my science and evaluate (favorably or unfavorably) other research. Working on Twitter/X specifically (given the character limit) has forced me to not only condense my findings, but also how to simplify the language while being precise and accurate about my results (including limitations). You can find my “master thread” of threads here.
Where Consumers Are Most Needed in Research and Policy
The examples above seem fairly minor in the grand scheme of things. Consumer involvement can benefit so many more areas of research and policymaking. The main areas that come to mind:
Toxicant and exposure studies: Many studies that claim to find that e-cigarettes produce high levels of harmful exposures involve using e-cigarettes in ways that are aversive and not representative of how people actually vape (e.g. “dry puff”). As a result, the harmful exposures are greatly exaggerated (Farsalinos et al. 2015; Soulet & Sussman 2022). Having consumers involved in these studies would strengthen the science and reduce the alarmism that is contributing to misperceptions about the continuum of risk.
Any studies recommending a policy: I’ve already covered the gist of this above in the section on “indirect effects” language. Many of the consumer advocates are (or were) vape shop owners and have seen firsthand how restrictive e-cigarette policies have negatively impacted their customers (see James Deighan’s post in the context of Utah’s flavor ban). Just about every academic paper ends with (whether supported by the study findings or not) a recommendation for policy or other public health efforts, e.g. marketing or packaging restrictions, graphic warning labels, messaging campaigns, and of course partial or complete bans. Consumers should have a platform for commenting on how these recommendations would affect them.
Product characteristics: Currently in the US, the FDA has only authorized tobacco-flavored and (less often) menthol-flavored e-cigarettes. But many, if not most, consumers prefer other flavors, and there is growing evidence that non-tobacco flavors might be more effective for stopping smoking (Selya et al. 2025; Klemperer et al. 2025). Similarly, while an illicit market is less than ideal, there’s evidence that disposables have reached more UK adults to switch away from smoking, who hadn’t tried or responded to other kinds of e-cigarettes (Tattan-Birch et al. 2022). People who are proposing restrictive policies should have a better understanding of what kinds of products are benefiting people who smoke.
Freedom of choice: Self-explanatory. I believe people should have a right to use substances if it doesn’t harm others and as long as they’re aware of the risks. Especially if they are reduced-risk products and will prevent using a more harmful product.
Most importantly, consumers should be completing this list. I am not, and shouldn’t be, an authority on this, and neither should researchers or policymakers. We need to normalize giving consumers a platform.
Fortunately, consumer involvement is another area that has notably improved over just the last few years. The Global Forum on Nicotine (for whom I have a minor scientific advisory role) has always embraced consumer attendance and participation (there’s even a designated outdoor vaping area!) but most scientific and regulatory conferences have not had anything like this until recently. Skip Murray has spoken (or is scheduled to speak) this year as a consumer representative at several conferences (e.g. E-Cigarette Summit, Tobacco Science Research Conference, and the Food and Drug Law Institute conference on tobacco and nicotine products).
I would love to see this become the norm, especially at the Society for Research on Nicotine and Tobacco. I’d also love to see journals such as Nicotine & Tobacco Research and Tobacco Control have a structure for consumers (perhaps as a dedicated type of article) to comment on published papers or write opinion pieces. This would be a great way to systematically disseminate consumer viewpoints to the scientific audience.
What else have I missed, or what should be different on this list? Comments welcome.
P.S. As I write this, I’m at the Vermont Center on Behavior & Health conference, and a speaker shared a relevant anecdote. In the early days of e-cigarettes, one researcher criticized them, saying “they can’t be called electronic nicotine delivery systems because they don’t work” [i.e. they don’t deliver nicotine]. This researcher then received “hate mail” saying yes, they do deliver nicotine effectively, and the researcher then recruited experienced vapers in their next study.
I appreciate your work. I agree it is important to bring both sides together. TC and THR are miles apart. Your idea to bridge the gap with politeness, science, and users experiences can only help. I was pleasantly surprised to see you cited Skip, Jukka, and my son, James.
Mike
Great article. I like reading about the evolution of your thinking on this topic. Thanks for sharing.